
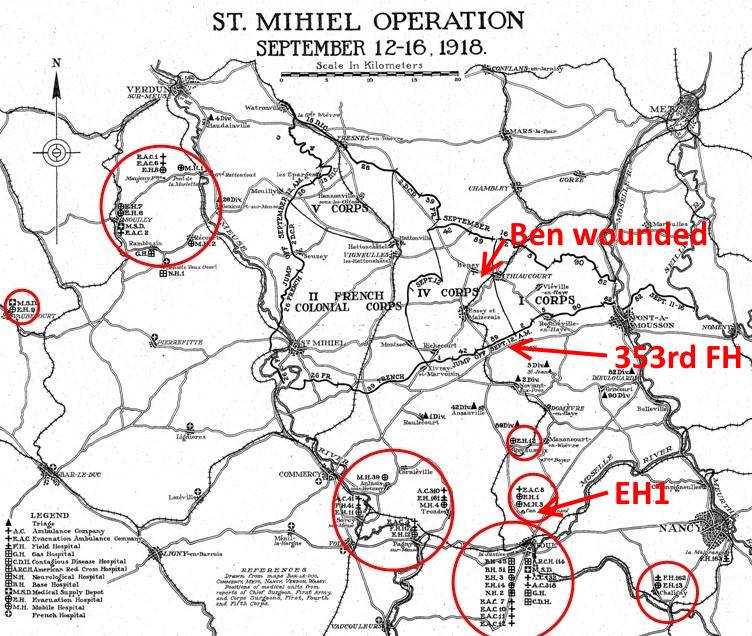
Ben Teply took a shrapnel wound in his right thigh on the afternoon of September 12.
Using his own records, some collateral info, and a bit of conjecture, we can follow his medical treatment.
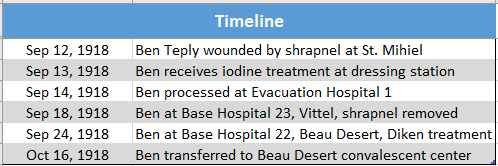
Where He Fell – September 12

A man’s treatment would begin with his own first-aid dressing, or help from his battlefield comrades.

Each man had two gauze bandages, two gauze compresses, and two safety pins. That sounds pretty feeble, but it was to prevent further loss of blood, and reduce the possibility of secondary infection.
If he was lucky enough to have stretcher bearers find him, they were trained in how to apply field dressings, control hemorrhage, splint fractures and to protect the wounded from gas.
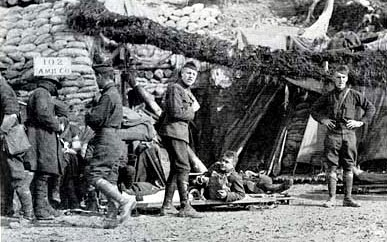
Aid Station
The injured soldier made his way to the aid station, either by stretcher or on his own or with help from comrades. The aid station would move every day or two in order to follow the progress of the battle line and be 500 to 1500 yards to the rear.
I’d guess that Ben couldn’t walk on his own. I think he would have been moved by stretcher to an aid station.
The aid station would deliver critical care
- Arresting hemorrhage
- Inspecting and readjusting the patient’s dressings and splints
- Administering morphine and the anti-tetanus serum
- Treating for shock and gas injuries
Then the aid station would try to move the patient to the rear to a dressing station.

Dressing Station
3000 yards to the rear of the aid station were the dressing stations.

The dressing station was similar to the battalion aid station in that it continued to provide emergency care.
At this level more sophisticated treatment could be carried out. Besides stabilizing patients, this facility had a continuous system of evacuation by ambulances from the battlefield to the field hospital for triage.
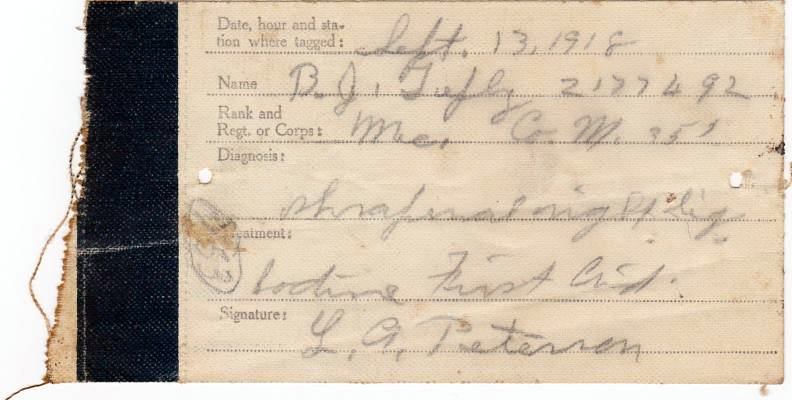
I believe this is where Ben’s field medical tag was assigned on September 13. If he was injured on the 12th, then it was a day before he arrived at the dressing station.
They treated his wound with iodine.
353rd Field Hospital
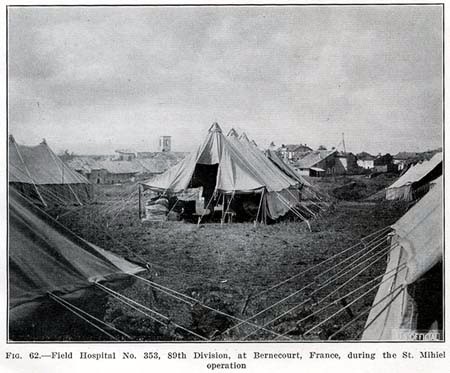
Two to four miles behind the line was the field hospital. It moved every few days to keep up with the line.
On September 13, the 353rd Field Hospital was near Bernecourt.

On September 13 four ambulances of Ambulance Company No. 353 got through to Bouillonville. The company had established a dressing station there. But on account of mud, bad roads across No Man’s Land, and congested traffic, it could not evacuate patients to the triage that night.

Next day 4 ambulances carried 16 litter patients to Bernecourt, and by evening of the 14th this company had transported 600 cases. One of these was probably Ben Teply.
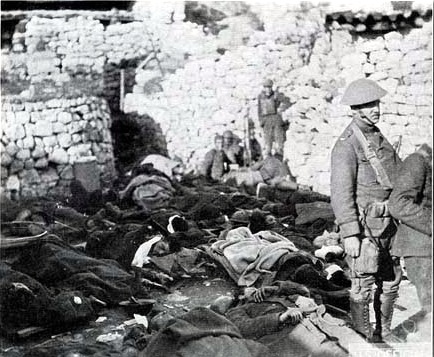
Triage
In 1918, the US adopted the French method of “triage”.

Triage is one of the most important concepts of battlefield care. It was probably formulated by Jean Larrey, the chief surgeon of Napoleon’s Grand Armée. Formally, it consists of dividing patients into three categories:
- Those who will recover with minimal or no care.
- Those who may die without immediate intervention.
- Those who are unlikely to live, regardless of treatment
Triage is a cold concept. It requires abandoning some patients to die, in order to spare resources for those who can be saved with reasonable effort.
The field hospital referred him to the Evacuation hospital, probably EH No. 1.
Evacuation Hospital
The Evacuation Hospital is 5 to 10 miles behind the line. It’s the last medical step under control of the attacking army.
You can see the Evacuation Hospital stamp that Ben was processed there.
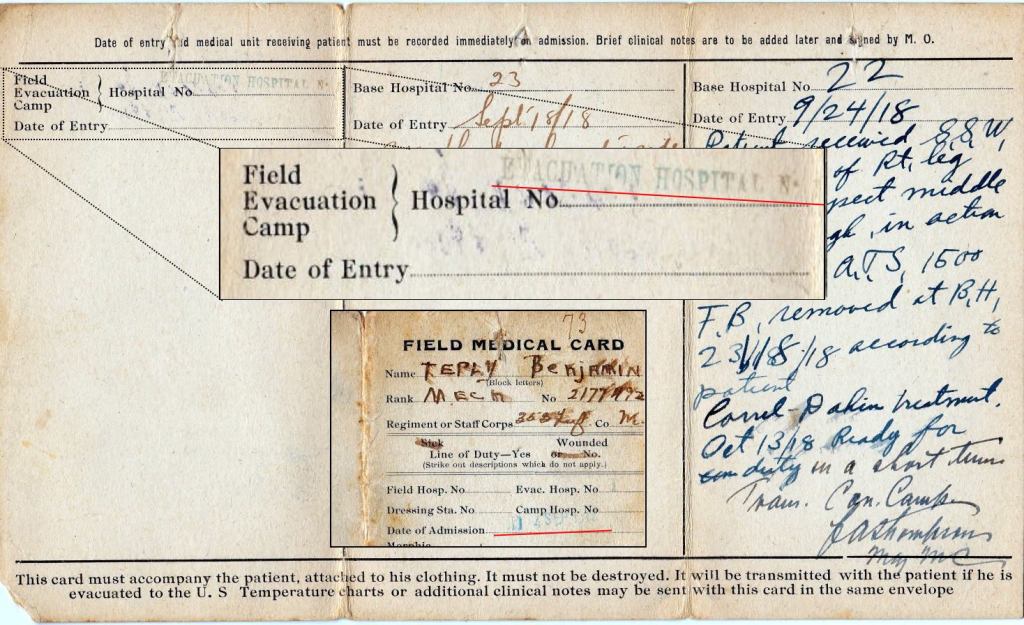
I think it’s Evacuation Hospital 1, and he was processed on September 14.
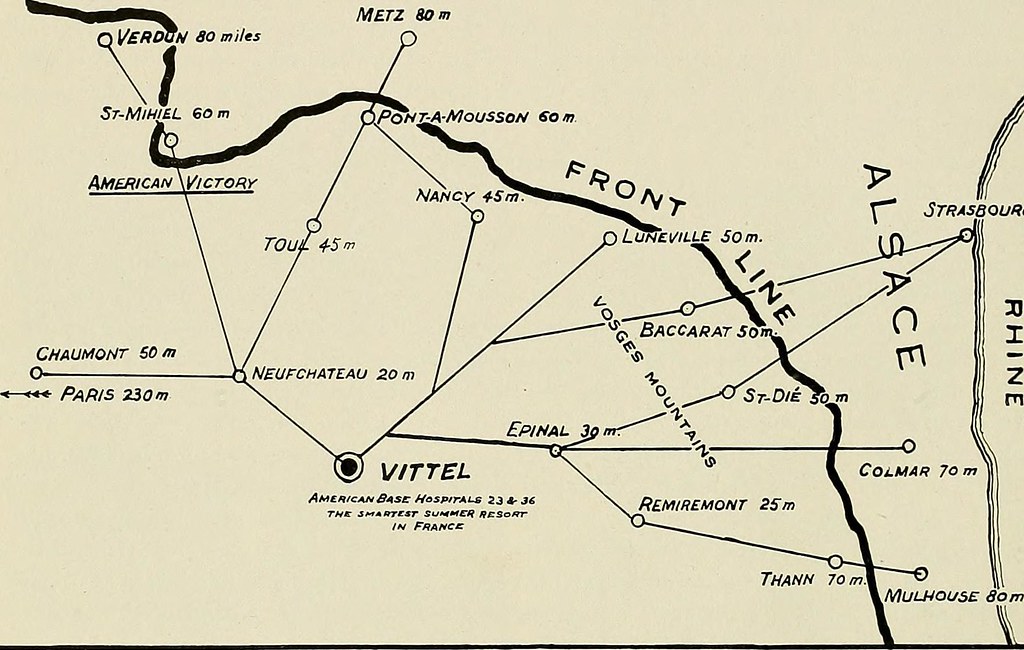
Base Hospital 23 – Vittel, Vosges
From evacuation hospitals, patients were sent by hospital trains to base hospitals located in the intermediate sections. There were 65 hospital trains.
Ben was transferred to Base Hospital 23, in Vittel.

Ben arrived on September 18, six days after he was wounded, and five days after his iodine treatment.
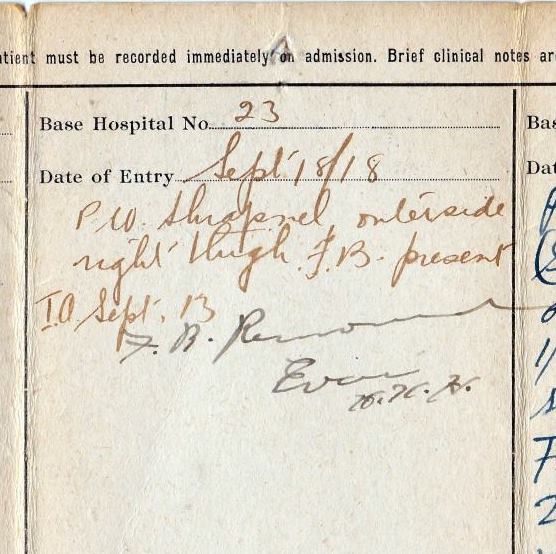
The medical record entry at BH 23 shows “P.W. Shrapnel, outerside right thigh. F.B. (foreign body) present. I.A. (In action) Sept. 13.”
And then “F.B. Removed”. (Foreign body removed.) So Ben had an operation to remove the shrapnel from his thigh, probably on September 18, the day he arrived.
Base Hospital 23 was about 60 miles southeast of St. Mihiel. So Ben was no longer in the command area of the 353rd. Base Hospitals were under command of Services of Supply (S.O.S).
Base Hospital No. 23 was organized in January, 1917, at the General Hospital, Buffalo, N. Y.
After arriving in France, the unit proceeded to Vittel, Department of Vosges, its permanent station, arriving there December 19, 1917. The hospital occupied in Vittel 21 buildings, with a bed capacity of 1,800, which could be expanded in emergency to 2,800.
A few days later, Ben was referred to another Base Hospital 22.
Base Hospital 22
Ben was transferred to Base Hospital 22, in Beau Desert. He arrived September 24.

We don’t know if he had infection, but he received Carrel-Dakin treatment. (See Nibbles Extra Credit)
On October 13, the surgeon reported that he would be ready for duty in a short time, and then transferred him to the convalescent center, which was at the same hospital complex.

Base Hospital No. 22 was organized in July, 1916, at Milwaukee, Wis., and was mobilized on January 7, 1918. It arrived June 22, 1918, in Beau Desert, Department of Gironde, and was the first hospital of a group that later became the hospital center.

The hospital had a bed capacity of 1,000, but during the stress of work in the fall of 1918 the hospital expanded to surrounding vacant units, until on November 10, 1918, 5,098 cases were under treatment.
The statistics for BH22 in October 1918, when Ben was there:
- Patients received………………………………………….5,448
- Returned to duty…………………………………………..1,332
- Transferred to other hospitals …………………… 449
- Average evacuated per day………………………… 175
- Forwarded to convalescent camps……………..1,282
- Deaths………………………………………………………………. 84
Beau Desert Convalescent Camp
Ben was transferred to the Convalescent Camp on October 16.



In the late fall of 1917, Beau Desert, in the vicinity of Bordeaux, was selected as the site for a hospital center, and construction began in December of that year. The site, about 5 miles west from Bordeaux and near the small village of Pichey, was a nearly level tract of land of approximately 550 acres.
The convalescent camp was organized late in July, 1918, and consisted of 25 wooden buildings and about 200 double hospital-ward tents, giving a capacity of about 4,500 beds, with a possible expansion to 8,000. The largest number ever accommodated was 3,800.
Nibbles Extra Credit
Carrel-Dakin Treatment
Ben received Carrel-Dakin treatment at Base Hospital 22.
Following is an article about the Carrel-Dakin treatment, quoted from “Delivery of Medical Care on the Battlefield – The United States World War One Centennial Commision – Medical Care in World War I“.
“The first principle of wound treatment is, and has been, debridement. This means cleaning the wound of all dirt and foreign matter, cutting out tissue which is too damaged to heal, and washing out the wound to remove dirt and debris too small to be seen.
Today, the surgeon has an array of antibiotics, which are used to irrigate the wound, and given systemically, to prevent and treat infection. During the Great War, antibiotics were still 20 to 30 years in the future.
The great advance of general anesthesia, however, was very well-established, permitting the surgeon to take enough time to properly clean and debride wounds.
Further, aseptic surgery was well-accepted, and practiced even on the battlefield. This avoids putting new bacteria in the wound, to further complicate healing. Even irrigation fluids were (and are) sterile.
Lacking antibiotics, surgeons used the older doctrines of antisepsis. A number of local antiseptics were available, including various preparations of iodine, phenol, alcohols, and, ironically enough, chlorine. The problem was to use something which would kill bacteria, yet not damage tissue.
The English-American chemist, Henry Drysdale Dakin, devised a solution of sodium hypochlorite, made initially by bubbling chlorine gas through a solution of sodium hydroxide or sodium carbonate.
It was not harmful to tissues, and even would help to “float” dead cells free of the surrounding tissue.
Working with the French-American surgeon Alexis Carrell, mentioned above, they developed the so-called Carrell-Dakin technique of wound irrigation.
To this day, the solution is still available as Dakin’s solution.
After the surgeon has debrided the wound, it is then irrigated with one or more liters of Dakin’s solution, some of which is left in the wound.
Open wounds were then irrigated with Dakin’s solution every three or four hours, or left packed with Dakin’s-soaked gauze. Military surgeons have long learned that trying to close battlefield wounds frequently resulted in closed wound infections.
Most battlefield wounds were left open for subsequent closure. Before the war, both Carrell and Dakin were in New York, and they may have developed the technique there. It was first used early in the war, when Maj Carrell was serving in the French Medical Corps.
The grim reality was that two-thirds of all casualties on the Western Front were produced by artillery shells. Machine guns and rifles used the same ammunition, and between them produced most of the rest.
Bayonet wounds were so uncommon that they were tabulated under “miscellaneous wounds” in the hospital log books.
Shrapnel from bursting artillery shells produces particularly ugly wounds, with a great deal of tissue damage and foreign material carried into the wound, including dirt from the trench environment. Frequently, the unfortunate soldier was also buried in the collapsed trench.”
Sources
- Ben Teply documents – Teply family memorabilia
- Much of the information – History of the 353rd Regiment, 89th Division, National Army, by Capt. Charles F. Dienst et al. – 1921
- Much of the information – Official Brief History of the 89th Division USA – 1917-1918-1919 – Maj. C.J. Masseck
- Information on Base Hospitals 22 and 23 – U.S. Army Medical Department – Office of Medical History – Chapter XXXIV – Base Hospitals –https://history.amedd.army.mil/booksdocs/wwi/adminamerexp/chapter24.html
- Delivery of Medical Care on the Battlefield – The United States World War One Centennial Commision – Medical Care in World War I – https://www.worldwar1centennial.org/index.php/delivery-of-medical-care-on-the-battlefield.html
- Photo of soldier arriving at field hospital – http://www.kumc.edu/wwi/index-of-essays/american-military-operations-and-casualties.html
- Maps of hospital movement – Google Maps

One thought on “52 – Ben Teply – WWI – Medical Treatment”